


[E3.3] How to Disrupt a Pandemic
Leverage large-scale "Hubs" to vaccinate the general public

Dear Reader,
In this Series, we have explored Wright’s Law [E3.1], operating leverage [E3.1], value networks [E3.2] and disruptive innovation [E3.2]. These topics are also relevant to tackling key healthcare challenges. To do so, we will first provide some background on the healthcare landscape and baseline conditions.
In this profile in Product | Strategy | Innovation, we will focus on 3 key topics to start a conversation on disrupting healthcare. The objective is to enable leaner, more efficient processes in key areas. Think early Tesla and its initial Roadster followed by the Model S to demonstrate competitive advantages of electric vehicles over internal combustion engines. Those early successes fostered Tesla’s journey to accelerate the transition to sustainable energy. We tend to look at healthcare as the totality of a multi-trillion dollar industry. We need to focus on a huge, total addressable market (TAM) like diabetes or obesity and disrupt that market first. Omada Health Co-Founder & CEO Sean Duffy represents this path starting at global design and innovation firm Ideo as a Health & Wellness Domain Specialist before starting Omada Health to take on pre-diabetes for diabetes prevention. Omada Health has now expanded beyond diabetes.
Three primary topics are presented in this profile.
Key healthcare challenges and opportunities
Access to care (Healthcare Providers, Employers, Consumers)
Vaccinating the general public to end a pandemic
Background
Healthcare impacts individuals throughout their life from birth until death. US Healthcare spending grew 4.6% in 2019 to $3.8 trillion or $11,582 per person. As a share of gross national product (GDP), this health spending equates to 17.7 percent. Other developed markets spend more in the range of 10-12% of GDP on healthcare. More details on that spending is a topic for another time, but one important feature is the non-linearity of healthcare spending across the US population. Personal healthcare spending data on a non-institutionalized population in 2009 showed 3% of healthcare spending was spent on 50% of the population with the lowest spending and 50% of healthcare spending was spent on 5% of the population with the highest spending.
Baseline
Healthcare is greatly influenced by a number parameters that would include an exhaustive list, but some of these factors that have a great impact are listed here. A baseline assessment across these parameters allows comparisons to innovations that optimize, simplify or disrupt that baseline state.
Scientific Evidence
Healthcare is supported by a strong foundation of basic science and clinical evidence to guide healthcare practice, diagnostic principles and therapeutic interventions with drugs and devices. Academic medicine plays a key role to advance the scientific evidence that leads to new technologies and investigational procedures.
Healthcare Providers & Practice Guidelines
Healthcare providers span specialties and primary care and licensed in the state where they practice. Practice guidelines help to standardize procedures, diagnostic criteria and recommended treatment pathways. Referrals to specialists may be required by primary care physicians by certain health benefit plans. Appointment availability varies by region and specialty, but routine primary care wait times can limit easy access in some cases. Telemedicine allows these providers to provide virtual care to their patients to improve access when needed.
Regulated Drugs & Devices
The Food and Drug Administration is responsible for protecting the public health by ensuring the safety, efficacy, and security of human and veterinary drugs, biological products, and medical devices; and by ensuring the safety of our nation's food supply, cosmetics, and products that emit radiation.
Health Benefit Plans, Claims & Processing
Health benefits plans expand the scope of what we traditionally refer to as health insurance. These plans can include other benefits such programs with fitness gyms, health & wellness, message therapy, acupuncture, counseling services, etc. Covered medical services may require a pre-authorization by the healthcare provide to the patient’s health benefit plan so the plan can review specified information to determine if the service will be covered. This process requires time by all parties involved to provide some controls over the covered services. Claims for covered services as also submitted by a healthcare provider to health benefit plans for reimbursement based on negotiated rates.
Health Systems & Infrastructure
Health Systems include Mass General Brigham, Cleveland Clinic, Mayo Clinic, Intermountain Healthcare, Kaiser Permanente and Geisinger Health are examples of health systems. Some are primarily hospitals, clinics and provider networks. Others like Kaiser vertically integrate health and medical services with their own health benefit plans just like Tesla approaches innovating end-to-end products and services direct-to-consumers to accelerate the transition to sustainable energy.
Telehealth, Retail Clinics & Consumer options
Teladoc, Amazon Care, Hims, Roman, Minute Clinic, Walmart Care Clinics, Warby Parker, Omada Health and Calm are alternative ways for consumers to access limited health services at 50-70% of the cost of conventional medicine with varying degrees of providers spanning physicians, nurse practitioners, optometrists, psychologists and health coaches. Telehealth in particular improves access by connecting consumers to virtual cash pay services. The coronavirus pandemic has accelerated the adoption of virtual care.
Social Determinants of Health (SDoH)
The SDoH include healthcare access and quality, education access and quality, social and community context, economic stability and neighborhood and built environment. Health systems and benefit plans are experimenting with public health programs that address affordable housing and other SoDHs under the assumption the these services save money over time.
1. Key healthcare challenges and opportunities
Healthcare in the U.S. represents a significant portion of GDP as mentioned in the background. Compared to other countries, higher prices for services in the U.S. are a key driver for higher overall spending. The administrative costs for healthcare per capita in the U.S. is also about 4x that of the average for other developed countries.
Challenges
Fragmented
High-Friction (limited access, pre-authorization, redundant processes, claims processing)
Expensive per capita care (US spends a lot less on social determinants of health and way more on medical care than other developed markets)
Chronic Disorders (mental health, diabetes, hypertension, obesity, heart failure, chronic pulmonary obstructive disease, asthma, substance use disorders)
Opportunities
Single payer, universal healthcare model that tenders services to private health benefit plans. This is analogous to how NASA has moved to competitive bidding with the private aerospace industry to resume human space flights with SpaceX and other companies.
Blockchain smart contracts to automate the validation of providers/health systems/patients identification and process pre-authorizations plus claims.
Differentiate care between solution shop hospitals vs. value-adding process centers. Solution shops can handle patients without a definitive diagnosis or needing uncommon clinical pathways. Value-added process centers optimize high-demand procedures for continuous improvement, enhanced quality and declining cost with cumulative unit procedures.
Precision medicine leveraging genomics to guide evidence-based treatment(s) with a definitive diagnosis.
Consumer triage (self-directed action plan based on symptoms, link to telehealth, virtual care to prescribe treatments for routine care)
Digital Health, Digital Medicine, Digital Therapeutics augment or replace conventional diagnostics and treatments.
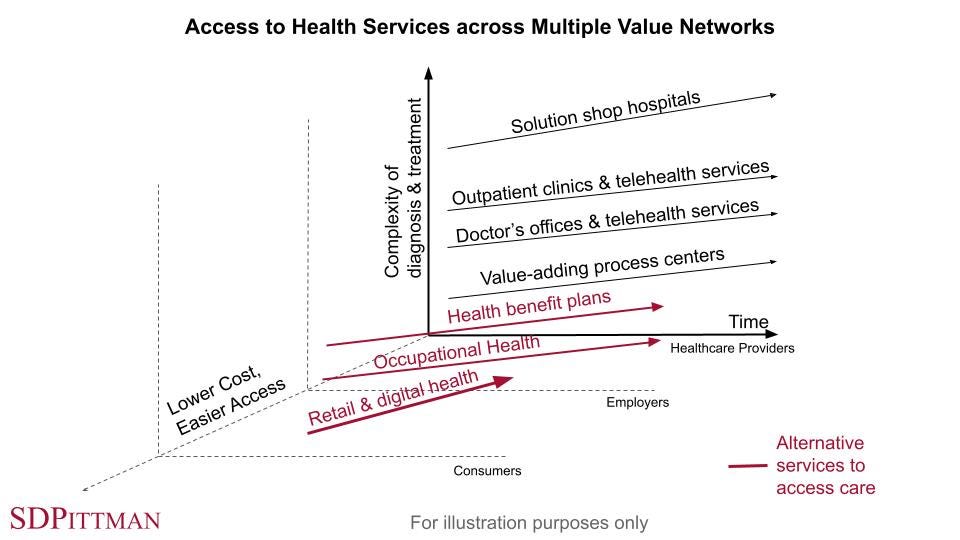
2. Access across multiple value networks
We discussed value networks in profile [E3.2]. These represent a business model and how the model works regarding regulations, suppliers and channel partners/distributors for a common class of customers. In healthcare, business models are influenced by reimbursement as the primary strategy to monetize regulated products, suppliers like hospitals and services provided by licensed healthcare providers. Health benefit plans construct & define services to employers to build a book of covered lives and monthly premiums to fund these plans. The health benefit plans then contract with hospital and provider networks to provide the defined services at negotiated rates to the covered lives under the plans. Government-sponsored programs like Medicare and Medicaid add additional covered lives to these hospital and provider networks. Individuals not covered by a health benefit plan or government-sponsored program have to pay extremely high prices to access these services without access to the buying power of participating in a plan. This creates demand for lower priced alternatives with business models that limit the use of reimbursement and healthcare providers.
In profile [E3.2], we demonstrated how multiple value works can be organized using a 3rd axis to segment based on cost and/or other variables. We showed for Apple products, how mobility helps differentiate multiple value networks. Regarding healthcare, a key way to differentiate value networks is how individuals access care because that impacts the sourcing of suppliers. Two key access points for care are health care provider channels and consumer channels. A third access point is through employers to form somewhat of hybrid since that is how many individuals and their family receive a health benefit plan. These individuals can also access a growing number of options provided to consumers with preferred pricing based on the size of their company. Health benefit plans competing for corporate accounts can cost-effectively bundle desirable health benefits outside the scope of covered healthcare services into a health plan to make it more attractive.
The 3 unique access channels are listed with some key features for each.
Healthcare Providers (HCPs): Licensed HCP networks within a state are available through hospitals, clinics, offices and telemedicine when a medical opinion, consult, prescription or surgical procedure is desired or required for covered medical services.
Practice guidelines and coordinated care match a definitive diagnosis to an evidence-based therapy and clinical outcome(s) to verify therapy meets the stated objective(s).
Solution shop hospitals provide a wide spectrum of medical specialists and services to handle almost any patient that presents with a wide spectrum of symptoms and needed services whether acute or a chronic condition. In many cases, this requires intuition by a trained physician to coordinate care and to work through various tests towards a definitive diagnosis. This helps determine recommended treatment(s). These hospitals see a high mix of conditions with patients distributed across many conditions resulting in lower volumes for the majority of required procedures. Leading hospitals in this category include the Mayo Clinic, Massachusetts General Hospital and Cleveland Clinic.
Outpatient Clinics and Doctor’s Offices are where a lot of care is provided to patients through office visits, diagnostic tests and procedures. This is where the bulk of primary care is provided. General Hospitals extend the outpatient clinics with inpatient services and more advanced procedures and surgical suites. Telemedicine provides remote access to these providers for convenience when this service is adequate to serve the need.
Value-added process centers provide a limited set of services compared to the solution shop hospitals. They specialize in areas where they can optimize process, controls and outcomes to attract a high volume of patients for specific procedures in high demand like joint replacement, cardiac catheterization and cataract surgery. These facilities have a very low mix of procedures and a high volume of patients going through the procedures they offer.
Shouldice Hernia Hospital outside of Toronto is an example of such a value-added process center. The founding surgeon, Dr. Edward Shouldice, developed a unique approach to treat abdominal hernias and opened his own hospital in 1945. The hospital performs approximately 7,000 hernia repairs annually with a 99% lifetime success rate repairing primary inguinal hernias.
Employers: Provide competitive options for health benefit plans that span coverage for medical services to health benefits employees can access vs. doing so as an individual consumer. Additional training, information and services can be provided by employers to employees as a health benefit.
Occupational health offers services to prevent and help manage workplace injuries. Physician extenders like nurse practitioners, physician assistants, physical therapists, occupational therapists, mental health providers, etc. can see employees onsite within the workplace for convenience and under the supervision of an off-site HCP to also help manage cost.
Consumers: Online tools can help consumers better understand their symptoms and rank available therapy options available as a consumer to try. Products and services available to consumers without a provider or prescription through retail and online channels. Mobile apps and digital solutions offer a range of services including digital health & wellness with varying degrees of evidence to support their use. Options to connect to area providers for a medical opinion, consult or conversion from consumer to patient provide significant value.

3. Vaccinating the general public to end a pandemic
A significant component to disrupting healthcare identifies evidence-based procedures in high demand that can be repeated in high volume with limited variability or mix. High volume, low mix procedures require evidence-based standardization (increases quality) and should be provided with a combination of medical and allied health providers to meet the demand. This model isn’t the Mayo Clinic where any patient enters the facility and can most likely be diagnosed and treated effectively with a combination of standardized and investigational procedures.
When demand is high, permanent or temporary “hubs” are created to bring patients and staff into one location to provide very limited mix, high volume services. Total joint replacement, cardiac catheterization and cataract surgery are examples of high volume procedures. But an even greater demand is only one procedure (administering the COVID-19 vaccine) needed for the the majority of the US population age 17-18 years or older as soon as possible. Synthetic mRNA vaccines have to be administered in 2 doses so that actually doubles the demand to administer those vaccines. The vaccination procedure should be the same for everyone, but the on-site services should adapt to all anticipated outcomes for at least 15 minutes after the the vaccine is administered. For most patients, they will experience the same outcome under an observation period with no event. But if a vaccinated patient does have an allergic reaction, medical providers or paramedics should be onsite to intervene for these events and to also provide a quick response if there are any unanticipated medical emergencies while patients are onsite.
Texas Motor Speedway launched a COVID-19 Vaccination Hub in Denton County just outside of Ft. Worth, Texas on February 2. The site was selected due to its ability to handle very large crowds of people and vehicles. The immediate daily goal is to batch up to 32 patients at a time using 16 vehicle lanes to provide 10,000 vaccinations per day averaging 1,000 per hour. The design is a drive through clinic with tents to administer the vaccine by trained allied health staff with medical oversight. An appointment is required and trained EMS staff are on-site for the required 15 minute wait after the vaccine is administered in case there is an allergic reaction. No walk-in patients are allowed to help drive efficiency. 400 fire, medical and volunteer staff are being used to operate the Hub.
That also means it is feasible to vaccinate 20,000 patients per day operating 24 hrs x 7 days a week using the same configuration. More lanes and more staff would enable even more vaccinations per day. Expanding on the Texas Motor Speedway Hub, the NFL has 30 Stadiums that can each handle approximately 80,000-100,000 football fans who park, tailgate and attend games August through January. These venues are in the vicinity of densely populated cities. Massachusetts Governor Charlie Baker announced on January 12, 2021 Gillette Stadium would provide the state’s first large-scale vaccination site operated by CIC Health. Fallon Ambulance provides vaccine preparation and administration services and Mass General Brigham provides medical oversight. This site is currently designed to serve 5,000 patients per day, but could scale up as needed. On February 3, 2021 the Boston Red Sox and CIC Health announced they had started a vaccination program at Fenway Park that will be able to administer up to 1,250 doses per day. This can scale as well for the general public with more staffing.
The Cambridge Innovation Center (CIC) builds and operates innovation communities around the world from Kendall Square in Cambridge, MA to Tokyo, Japan and Rotterdam, Netherlands. The CIC was significantly impacted by COVID-19 with resident-companies having to work remotely. As the CIC started planning for these companies to return to work, they realized COVID-19 testing was not readily available. So the CIC founded CIC Health and partnered with Ariadne Labs to form the Assurance Testing Alliance (ATA) to help create the infrastructure to expand COVID-19 testing and contract with laboratories like the Broad Institute of MIT and Harvard to run the PCR tests. The ATA currently has the capacity to run up to 2 million COVID-19 tests per month with adequate logistical support. CIC Health offers assurance testing in the communities where they have a presence to individuals, organizations, and currently 120 schools in New England. CIC Health recently expanded it services to include COVID-19 vaccinations previously mentioned at Gillette Stadium and Fenway Park.
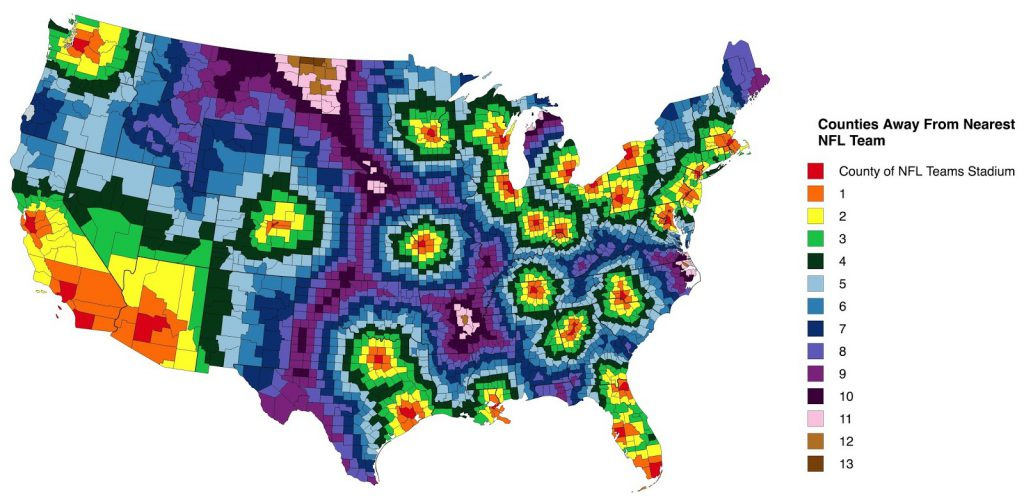
This heat map shows how many counties away each county in the U.S. is from an NFL stadium (Note: this map was constructed before the Raiders moved from Oakland to Las Vegas and the Chargers moved from San Diego to Los Angeles). This network of NFL stadiums can be augmented in areas maybe 6 counties and greater away from an NFL stadium with other venues like college or county stadiums, arenas and even Walmart parking lots in rural areas. The idea is to create a national network of Hubs with the fewest number of sites for the general public to receive a coronavirus vaccine. Large-scale vaccination at few sites also streamlines logistics and distribution to reduce the units of vaccine in transit or inventory waiting for use. The impact is a synthetic increase in available supply to vaccinate patients.
This network of 30 NFL stadiums might be able to cover 50% of the US population with access to transportation. Additional sites that increase the total number of Hubs to 100 locations could provide access to maybe 85% of the population who have access to transportation. Densely populated cities also have a significant number of residents who do not have access to transportation. These residents could be transported to a Hub for vaccination. However, additional mini-Hubs or mobile EMS teams would also be needed within communities due to the importance to protect these groups due to the higher coronavirus risk in these groups. These inner-city residents should be provided both options to minimize substandard care.
The NFL has a substantial budget and benefits significantly by accelerating the end of the pandemic so operations can resume to more normal conditions. Therefore, these organizations should provide these services at limited cost to local, state and federal governments and the US taxpayers. The positive public relations impact should also help offset these costs. On February 5, 2021, the NFL offered all 30 stadiums to U.S. President Joe Biden for use as large-scale coronavirus vaccination Hubs.
So what is the potential impact of 100 COVID-19 Vaccination Hubs around the country without any supply constraints on the vaccine, accessories or staff over a 5 month period from April-August 2021. If each Hub could operate 24x7 to administer an average 20,000 vaccine doses per day, 7 days per week for 20 weeks, we could administer 14 million doses per week or 280 million over 20 weeks. Assuming each person needs 2 doses, 140 million patients would be fully vaccinated with this plan. The J&J vaccine will require only one dose once approved, so that could be used to help boost full vaccination throughput to 200 million individuals over the 5 month period.
Coordinating each individual’s vaccination appointment date/time at each site and CDC COVID-19 Vaccination Record (vaccinated individual’s name/birthdate, 1st/2nd/other dose, date of administration, site, vaccine manufacturer, vaccine lot number) can all be handled with a mobile app, web dashboard and cloud services. This could evolve into a personal health record to document all vaccinations throughout an individual’s life. The personal health record can be shared with healthcare providers, schools, employers and others. Amazon, Apple, and Google would likely provide this as a public service. Uber and Lyft could also support transportation services for vaccinations due to the national attention for 100 large-scale COVID-19 Vaccination Hubs.
Current Status of COVID-19 Vaccination Campaign
The U.S. is working to vaccinate a high percentage of its population against COVID-19 as soon as possible to help end the pandemic. Since the vaccine distribution began in the U.S. on December 14, the NPR COVID-19 Vaccine Tracker reports more than 44 million doses have been administered reaching 10.2% of the total U.S. population according to the CDC as of February 11. Herd immunity to counter the pandemic is estimated to require vaccinating 60-70% of the population based on the infection rate and efficacy of available vaccines. That equates to 197 - 230 million of the U.S. population. Thus, our Hub model to vaccinate 200 million individuals with 100 COVID-19 Vaccine Hubs would be in scope to achieve herd immunity over the 5 month period, but with a portion of the population already vaccinated and additional sites vaccinating individuals, herd immunity could either be achieved sooner or with less throughput per Hub to meet the stated objective over 5 months. That translates into options.
Operation Warp Speed is a public-private partnership initiated by the U.S. government to facilitate and accelerate the development, manufacturing, and distribution of COVID-19 vaccines, therapeutics, and diagnostics. The program was officially announced on May 15, 2020. It is headed now by co-chair of the COVID-19 Advisory Board and past FDA Commissioner, David Kessler. The program shown in Fig. E3.3-4 was initially funded with about $10 billion from the CARES Act (Coronavirus Aid, Relief, and Economic Security) and is a key reason the U.S. had multiple COVID-19 vaccine candidates on accelerated timelines for development, clinical research, FDA approval and scaled production.
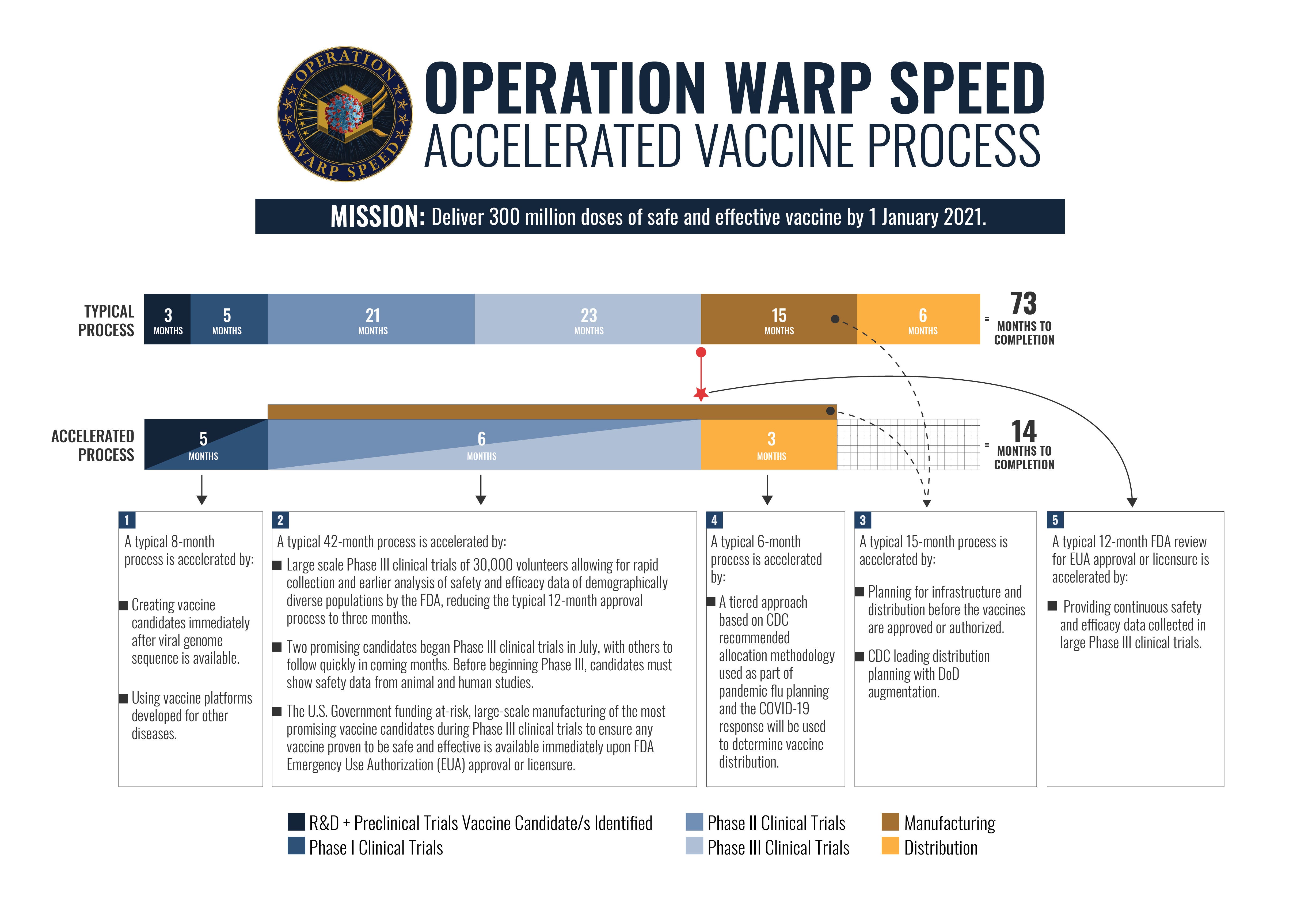
Operation Warp Speed also took steps to build manufacturing infrastructure, distribution and controlled product inventory during clinical trials, FDA submission and FDA review vs. after the clinical trials were completed to validate the product before moving forward with an FDA submission for review and hopefully approval. That means Operation Warp Speed released funds at risk to start manufacturing and production at-risk. It also means if a clinical trial failed, the manufactured product would have limited to no commercial value. This at-risk production helped build inventory for distribution to administer 44 million doses to date in the U.S.
Operation Warp Speed worked with the CDC to prioritize certain groups for the initial release of vaccine across the country. Distribution maximized the use of existing pharmaceutical distribution infrastructure and established a Central Distributor for kitting and coordinating distribution operations. IT infrastructure supports end-to-end ordering, distribution, administration and tracking. Where challenges arise is when bulk deliveries from centralized inventory have to be broken into much smaller quantities to ship to many vaccination sites who vaccinate dozens to hundreds of individuals per day. When a vial of vaccine is opened it also has to be used within a few hours. If there are no shows for vaccination without an adequate queue of individuals waiting, vaccine doses risk being discarded. This is a significant risk when too many sites are vaccinating limited numbers of patients and good doses are discarded. This is risk is eliminated with our model for large-scale vaccination at 100 Hubs around the country. There will always be somebody in the queue by design to fill the slot for a no-show.
Conclusion
The U.S. has one of the most advanced healthcare systems in the world for acute care, rare diseases, academic medicine developing investigational diagnostics and therapies, and other key areas. But U.S. healthcare is also the most expensive in the developed world by a large margin with close to 18% of gross domestic product (GDP) going towards healthcare. We grossly underspend on social determinants of health compared to other developed markets and overspend on chronic disorders and diseases like diabetes, congestive heart failure and hypertension. The U.S. also faces large societal issues like mental health, substance use disorders and obesity that are expensive to manage only through health care providers.
Disrupting healthcare does not mean changing everything. It means exploring what we have already presented in Product | Strategy | Innovation like Wright’s Law, value networks, low-mix/high-volume procedures and leveraging platform technologies across multiple value networks. Accelerating vaccination for the US general public to control a pandemic is not a routine use case, but it highlights what disruption looks like using available resources inside and outside of healthcare to optimize a high-volume process like an Amazon, Tesla or Apple.
When the pandemic is over and we look back on the lost lives, lost economy, lost jobs, lost businesses, stressed healthcare system and cost to mitigate an uncontrolled virus, we will likely identify at least 4 areas that need to be addressed. 1.) Early activation of personal protective equipment (PPE) manufacturing was the big miss to overcome supply shortages. Wearing masks by the general public was likely not encouraged because PPE was in such critical supply shortages for healthcare workers, but is a standard precaution now in addition to social distancing to reduce infection risk. 2.) Reliable COVD-19 testing with a fast turnaround is widely available to help catch and mitigate outbreaks. 3.) Social distance monitoring and contact tracing using technology to track contacts with other individuals in case a positive case is diagnosed allows these potential infections to be isolated for a specified amount of time to reduce infection risk and 4.) Tackle social determinants of health like reliable access to housing, income, food, education, healthcare, etc. to improve public health.
We will explore value networks to access care through providers, employers and consumers in future profiles. A key opportunity to disrupt fragmented and inefficient areas of healthcare is to span these different value networks with common digital platforms to connect consumers to providers when needed and to build compelling solutions for employees through their employer.
If you are not a subscriber, please consider doing so to get updates on this topic and more.
If you liked this post, please share with your networks so others can benefit, too.
Nothing in this post is intended to serve as financial advice. Do your own research.